


Crohn’s Disease is an illness in which inflammation develops in parts of the gut leading to symptoms such as diarrhoea, abdominal pain and tiredness.
The inflammation can be mild in many cases but can sometimes be severe requiring strong medication or an operation to remove an affected part of the intestine. Crohn’s Disease is one of the two conditions known as Inflammatory Bowel Diseases (IBD); with the other being ulcerative colitis. The symptoms and effects are similar to those of gastroenteritis (food poisoning) but differ in that they are not due to an infection and persist for a long time or until treated.
Who gets Crohn’s disease?
The disease affects mainly young adults but can affect teenagers or younger children and can sometimes start later in life. Men and women are affected equally. Crohn’s Disease affects about 1 in 1000 people (most people know one person affected by the condition). Crohn’s Disease and ulcerative colitis can run in families – about one-fifth of people with the condition will have another family member affected.
What causes it?
It is thought that Crohn’s Disease develops as a result of the immune system in the intestine reacting abnormally to bacteria at the surface of the gut. This abnormal immune reaction is likely to be inherited with a number of genes that may contribute to causing Crohn’s Disease having now been identified, which are mostly involved in how we handle bacteria in the gut. It is still not known if one, a few or many types of bacteria are involved. Other factors affect the chances of getting Crohn’s Disease, with smoking being the most important risk factor. Many patients ask whether there is a dietary cause but there is no firm evidence of this.
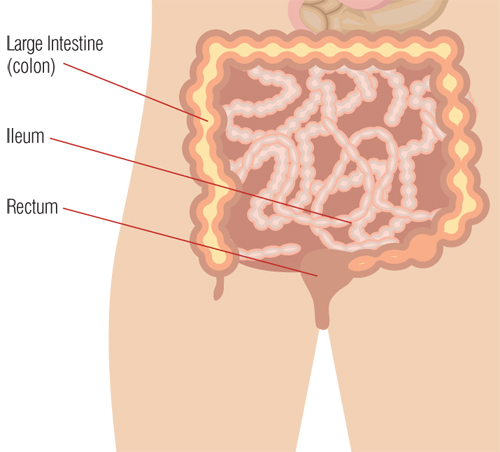
Which part of the body does crohn’s disease affect?
Any part of the gut can be affected in Crohn’s Disease. The most common area is the last part of the small intestine (terminal ileum) and the first part of the large intestine (or ‘colon’), near the appendix. In some people, only the colon is affected, in a pattern similar to ulcerative colitis. In others, multiple parts of the gut are affected. Rarely, the mouth, gullet or stomach may be involved. However, in some people, the inflammation in the gut also triggers inflammation outside the intestine leading to arthritis, eye inflammation or skin complaints.
How does Crohn’s affect the intestine?
One form of Crohn’s Disease results in patches of inflammation in the lining of the intestine with groups of small ulcers, similar to mouth ulcers. In moderate or severe Crohn’s Disease, these ulcers become much larger and deeper with a lot of surrounding redness. The inflammation can make the intestine become thickened, blocking the passage of digested food. In some cases, deep ulcers break through the wall of the intestine causing infection outside the bowel (an abscess) and this can then spread to the skin or a nearby part of the body. This is known as a fistula. These most frequently occur around the anus. As the inflammation heals, scar tissue may form which can in some cases also lead to a blockage in the intestine.
What are the symptoms?
The main symptoms of Crohn’s Disease are diarrhoea and abdominal pain. There may be some blood or mucus in the faeces, especially when the lowest part of the gut is affected. Digested food or faeces building up in narrowed or inflamed areas often occurring an hour or so after eating usually cause the pain. Sometimes, there is a tight blockage in the intestine causing severe, griping abdominal pain after eating, with swelling of the abdomen and vomiting. Losing weight is common when there is a lot of inflammation, as eating causes pain and many people with the condition feel excessively tired. Some people also have a temperature or sweats at night. There may also be sore, red eyes, swollen painful joints and skin rashes. Some patients get perianal Crohn’s disease which means that the inflammation occurs around the lower bowel and anus.
How is it diagnosed?
When someone visits their doctor with symptoms of persistent diarrhoea and abdominal pain, they will try to decide whether special tests are needed to look for the possibility of Crohn’s Disease and ulcerative colitis. There are many causes of diarrhoea in young adults including the irritable bowel syndrome (IBS), and infection (for example after travel abroad). The doctor will listen to the symptoms and ask about any of the related symptoms described above and also whether there is anyone in the family with Crohn’s Disease or ulcerative colitis.
An examination will then find out if there are any signs of inflammation (such as tenderness in the abdomen or a lump) and whether there are any general signs of illness such as looking pale or underweight. A blood test might be arranged to see if there are changes in the blood, which suggest inflammation. If the doctor suspects that Crohn’s Disease is a possibility, a referral will be made to a specialist for further tests.
Which tests are used to diagnose crohn’s disease?
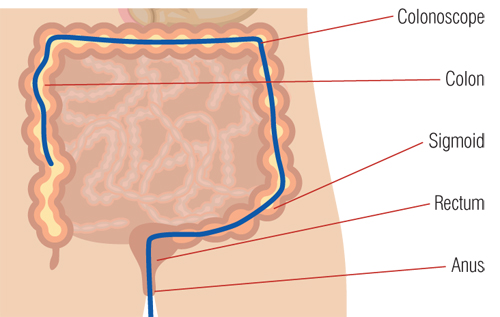
The most frequent test used to diagnose Crohn’s Disease is a colonoscopy. This involves the passage of a tube with a video camera at the end around the colon and, where possible, into the last part of the small intestine. Laxative preparation is needed before the examination to clear the bowel and allow good views of the lining of the intestine. In most cases, sedation is given through a vein at the start of the procedure to minimise some feelings of discomfort associated with passage of the tube along the colon.
By doing this test, doctors can get very accurate pictures of the state of the lining of the intestine and take samples for examination in the laboratory. If the colon and last part of the small intestine are seen to be normal, Crohn’s Disease is very unlikely to be present.
In some cases, other tests are also needed. For example, a barium follow through examination allows the whole of the small intestine to be shown. In this test, liquid barium is swallowed and X Rays are taken as it passes through the intestine. Increasingly, other methods are used; these include magnetic resonance imaging (MRI) or capsule endoscopy, where a radiopill is swallowed and transmits pictures as it passes through the intestine. Scans such as ultrasound or CT scanning may be needed, especially if an abscess or problems on the outside of the intestine are suspected.
How is Crohn’s disease treated?
Treatments for Crohn’s Disease aim to reduce or heal the inflammation in the intestine and to deal with the effects of the disease, such as weight loss, and any complications. The inflammation is generally treated with medicines but in some cases surgery is required to cut out very inflamed or narrowed sections of intestine.
Many patients ask whether they should change their diet, but there is no proven specific diet for Crohn’s Disease. There are, however, diets for certain situations. The most frequent dietary change is a reduction in fibre and indigestible foods, which cause pain when there is a narrowing in the intestine (a ‘low residue diet’). Specialised liquid formula diets (‘elemental’ or ‘polymeric’ diets) are also used as treatment in Crohn’s Disease, especially when it affects the small intestine. These diets rest the bowel, improve nourishment and reduce inflammation and are used especially in children where maintaining growth and weight is very important.
Medicines used to treat Crohn’s Disease are mainly directed at the immune system in the intestine.
- Antibiotics (such as metronidazole) can be helpful, either by reducing the bacteria, which ‘drive’ the inflammation, or to treat abscesses. They are not used for long-term treatment.
- Aminosalicylates are a relative of aspirin and are used to treat milder inflammation or reduce the chances of recurrence (for example, after an operation). Not all patients are helped by these drugs.
- Steroids (prednisolone, hydrocortisone) are much stronger drugs used to suppress inflammation when the symptoms are more severe. Steroids are very effective (about eight out of ten patients have a good response) but have side effects such as weight gain, insomnia, infection and acne and prolonged use can result in thinning of the bones. Steroids are therefore only used as a short-term measure to get Crohn’s Disease under control. There is a newer form of steroid (budesonide) which has fewer side effects due to mostly acting within the gut itself.
- For long term steroid use, immunosuppressive drugs are often used to reduce inflammation over a longer period and allow steroids to be stopped. Azathioprine and 6-mercaptopurine are the most frequently prescribed and around two-thirds of patients have a successful response. Side effects can occur and patients on these drugs therefore need to have regular blood tests. On the whole, however, most patients tolerate the drugs well and they remain the most effective medicine for keeping Crohn’s Disease under control.
- Methotrexate is another immunosuppressive drug, commonly used for treating rheumatoid arthritis. This is usually the next choice if azathioprine or 6-mercaptopurine have failed.
The strongest drug treatment used for Crohn’s Disease involves ‘biological therapy’ in which specially developed antibodies are used to block the effects of the molecules that are involved in the inflammation in the gut wall. The best-known biological therapies target a substance called tumour necrosis factor (TNF) and are given by a regular intravenous drip or an injection under the skin. Other similar treatments, which target different inflammatory mediators, are under development. These treatments are very effective but can also have side effects, especially increased rates of infection and allergic reactions, so they are reserved for people with severe Crohn’s Disease and when other medicines have not worked. They need to be used under care of hospital specialists.
Surgical operations are a very important part of the treatment of Crohn’s Disease and it is estimated that as many as eight out of ten patients will require an operation at some stage in their life. The main reason for needing surgery is to remove thickened blocked segments of the intestine. Medicines are unlikely to help these and an operation to cut out a short section of affected intestine is usually very successful with few problems and restores full health quickly. Sometimes, colonoscopy can be used to open up narrowed sections (with special dilating balloons) but this is only possible in certain cases. Surgery is also needed when badly affected parts of the intestine have caused an abscess or fistula. Such fisula can occur on the abdomen or in the perianal area. An operation can sometimes be the best option when severe Crohn’s Disease is not responding to drug treatment.
Does surgery mean having a stoma bag?
Many people presume that surgery for Crohn’s Disease means having a permanent stoma bag. In fact, stomas (ileostomy or colostomy) are not often needed and are nearly always a temporary measure9. After a section of affected intestine has been removed, a very delicate join (or ‘anastomosis’) is made between the unaffected ends of the intestine. In order to protect this join while it heals, the surgeon will often make a temporary stoma above, which is then taken away at a second smaller operation a few months later. This is done particularly when someone is underweight or taking steroids which reduce the ability of body tissues to heal.
Does Crohn’s disease come back after surgery?
Yes as there is no cure for Crohn’s Disease so it does come back, often in the section of intestine just above a surgical join. However, despite this, most people have no problems for many years after their operation. Recurrence is two-times more likely in smokers compared those who do not smoke. Drugs such as aminosalicylates or azathioprine can also reduce the chances of recurrence.
Does Crohn’s disease affect my chances of having children?
Overall, Crohn’s Disease does not have a significant effect on the chances of becoming pregnant or carrying a baby. In a small number of cases, inflammation or infection in the pelvis, or surgery to this area, can affect the ovaries, fallopian tubes or uterus reducing fertility. The commonly used drugs used in Crohn’s Disease are safe during pregnancy. It is always best to talk to your specialist if you have Crohn’s Disease and are planning a pregnancy or already pregnant.
Can I expect a normal life if i have Crohn’s disease?
In most cases, Crohn’s Disease does not have much impact on daily life, the ability to work or to enjoy an active social life, but does take some getting used to. When it is active, symptoms such as diarrhoea and abdominal pain often require time away from work, college etc and make it difficult to cope at home or go out. However, treatment usually makes the symptoms better within days or weeks so work and home life is restored quite quickly.
The chances of dying if you have Crohn’s Disease are no different to if you don’t have the disease. There are many forums and support groups around for those who suffer from Crohn’s Disease to join, help and find out more information from. One example is www.crohnsforum.com
What can be done to prevent Crohn’s disease?
There is currently no evidence any particular change in diet or lifestyle can prevent Crohn’s Disease. Not smoking, or stopping smoking, is perhaps the most important of all the things to do. Although not proven, it makes sense to eat a balanced healthy diet favouring freshly cooked food over processed foods.
What research is needed?
The cause of Crohn’s Disease remains unknown. However, our understanding of how and why the condition develops is increasing all the time. In particular, researchers are looking into how the hereditary (genetic) aspects of Crohn’s Disease might change the way the immune system in the intestine deals with bacteria and other dietary substances present at the surface of the gut. This is very important research and there is hope that it will, before too long, lead to much better treatments and maybe even a cure.
 The information on this page about Crohn’s disease is based on the leaflet produced by CORE (a charity fighting gut and liver disease).
The information on this page about Crohn’s disease is based on the leaflet produced by CORE (a charity fighting gut and liver disease).